| Assisted Hatching is another laboratory procedure which enhances pregnancy rates in certain women undergoing IVF. A small opening is made in the shell surrounding the embryo just prior to transfer of the embryo into the uterus. This increases the likelihood that the embryo will implant into the wall of the uterus resulting in a successful pregnancy. AZH maybe recommended for women who have elevated Day-3 FSH level or those who have failed IVF > 2 times and embryos having thicker zonas.
Microembryonic hatching is the technique in which the embryologist creates microscopic holes in embryonic shell to facilitate easier release of the embryo into endometrial cavity that improves implantation. Under a high-powered microscope, a small, slit-like opening is mechanically created using a fine glass needle while the embryo is held by gentle suction. Breeches are made in ZP of early cleavage embryos. Removal of necrotic blastomere from frozen, thawed, partially damaged embryo improves implantation rate.
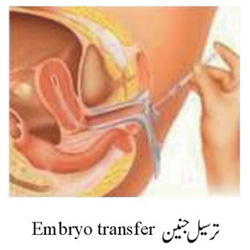
Embryo Transfer (ET): Empbryo Transfer done 3-5 days following egg retrieval is a simple procedure that takes less than 10 minutes and does not require anesthesia. The woman after undressing lies in Lithotomy position with full bladder. Cervix is exposed with bivalve vaginal speculum. Cervical mucus is cleared by gentle aspiration. |