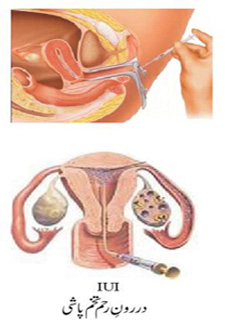
A thin plastic catheter is inserted into cervix. It is pushed onwards beyond the cervix so that t he tip of the catheter is in the uterus near the tubal openings. It usually passes easily. In case of difficulty the cervix is caught and pulled a little to correct the angle of flexion. It makes the entrance easy. Rarely if cervix is stenosed, a uterine sound may need to be passed to open it.
The syringe filled with the sperm is attached to the end of the catheter and the sperm sample is pushed out of the syringe under light pressure. It travels through the catheter to the uterus.
In natural intercourse only a fraction of the sperms make up the woman’s genital tract. IUI increases the number of sperm in the fallopian tubes (place of fertilization) by shortening the passage. Only the good spermatozoa reach there with their much-required energy conserved for the penetration of the ovum. They approach the ova without consuming their energy; therefore even weaker sperm may be able to fertilize the ovum. For many couples, this is less invasive and more affordable than IVF. It can be an alternative to IVF only if woman’s reproductive organs are healthy and the oviducts are open and functional.
Most women consider IUI to be fairly painless. There can be some cramping afterward, but what is felt is ovulation-related rather than from the IUI. The catheter often isn't felt because the cervix is already slightly open for ovulation.
Complications of IUI are infrequent. They can include infection, and brief uterine cramping.
Success rate in IUI is 10-15%. IUI helps in most of the cases if there is no biological barrier. If the woman is not pregnant after three IUI attempts, the next step is usually IVF-ET.
|