|
The size and shape some defects of uterine cavity can be judged and some of its defects detected by Hysterosalpingography. Hysteroscopy is comparatively new technique which had general acceptance in the last decade of 20 th century. It is used for the diagnosis and the treatment of intrauterine lesions. The woman is placed in the Lithotomy position. A Collin’s bivalve vaginal speculum is passed gently to separate the anterior and posterior vaginal walls to expose the cervix. Modern Hysteroscopes are quite narrow (2-4 mm diameter) and are passed through the cervix usually without dilatation. The uterine cavity and the tubal ostia are seen. Only rarely minimal dilatation is required if the cervix is stenosed or is nulliparous. As the dilatation is not required, the diagnostic procedure is done without anesthesia. If dilatation is required Para cervical block is given. In hypersensitive women, light sedation is used. |
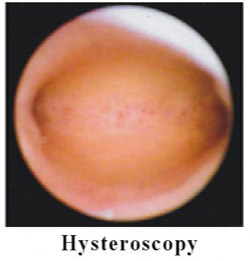 |
Uterine cavity is distended with carbon dioxide or suitable fluids. The uterine cavity is illuminated and its inside visualized. In fertility evaluations the size, shape, the lining of the uterine cavity, and the tubal ostia are studied in detail. It is essentially used in abnormal uterine bleeding to locate the cause of it. Even the treatment of intrauterine lesions is done through the vision of hysteroscope. Many abdominal operations have been avoided and uteri saved by the use of Hysteroscopic techniques of intrauterine surgery.
Evaluation of female reproductive passages It is important both in men and women that the ovum and the sperm reach the site of fertilization, the oviducts.
For natural conception to take place, the passages of both need to be patent, healthy and functional. Sperms have to pass through the epididymis and the ejaculatory ducts in the male to be deposited in the vagina at the time of ejaculation. It is easy to know about the male passages by just finding the sperms in the semen analysis and PCT. Vasography is used to detect the obstruction of vas deferens male.
In female sperms ascend through cervix and the uterus on to the oviducts. Ovum just goes to the oviducts after release, but as it is immotile, it has to be helped.
Evaluation of female passages is invasive requiring a procedure to enter the reproductive passages. The female reproductive passages should be patent for the ova and sperms to reach site of fertilization in the fallopian tubes. These tests are wrongly known as tubal Patency tests because areas from cervix to peritoneal ends of oviducts are assessed. The female passages extend from vagina, through cervix uteri, the body of the uterus, and the oviducts on either side of the uterus into the peritoneal cavity. |
 |
There can be infection and other risks that can create fertility problems. Patency tests should be carried out by experts with care against infection. It is advisable to do these after the ovulation and sperm production as been tested and even treated.
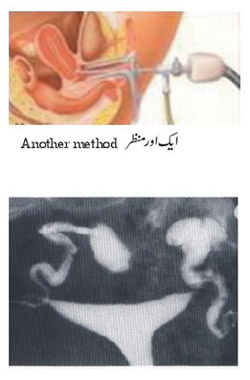
General principle is that a canula or catheter is introduced into the uterine cavity passing through vagina and the cervix. Some detectable liquid is pushed through this canula under mild pressure and its evidence seen in the pelvic cavity. Dye in the uterus, fallopian tubes and the free spill in pelvic cavity indicates Patency of passages. This is detected by
- Hysterosalpingography(HSG) if radiopaque dye is used and seen by X-rays;
- HysteroSonogrpahy(HyCoSy) if sonopaque dye is used and seen by ultrasound;
- Pelviscopic Dye test by passing a colored liquid, Methylene Blue and seen directly by pelviscope.
There is not much to choose between X-rays and ultrasound tests, both of which are done as outpatient procedure. X-rays has the benefit that a film is always taken for record and is comparatively cheap. Ultrasound test called echovist is four to five times more expensive than the X-rays test.
Pelviscopy has advantage that any membranous adhesions around the tubal opening, which can hinder the access of the ova to the tubal opening, endometriosis, uterine and ovarian lesions in the pelvis, can also be detected by it. This makes the pelviscopy evaluation superior to other methods.
Pelviscopy should be the first choice for evaluation of patency of reproductive passages. If the Methylene Blue test is negative, i.e. the dye is not visualized in pelvis; HSG should follow to locate the site of the blockade. A composite approach doing pelviscopy, hysteroscopy and endometrial biopsy gives complete evaluation.
Old fashioned gas insufflations tests are still done by many in developing countries especially by unqualified persons. It does not give any useful information, mostly is misleading and should never be done.
|









