Gynecological Endoscopes; Pelviscopy and Hysteroscopy The modern concepts and technology have revolutionized the gynecological practice. Introduction of endoscopes, the developments in optics and close circuit vision technologies are among the gifts of the twentieth century. Recent advancements in visuals expanded the use of endoscopes in medical practice for diagnosis and therapeutic procedures. Micro-endoscopes, with very small diameter have further simplified the diagnostic techniques as the small diameters allow them to pass through without discomfort as a result their use is most convenient for the day care outpatient procedures.
Endoscopes have made distant body cavities accessible. They are small tubes in which optical lenses are arranged in such a manner that small and remote areas in the body can be approached through small entry points and illuminated from distant light sources. These narrow steel tubes are shaped for the particular organ and the endoscope named accordingly. Light passing through lenses in the endoscope is intensified brightening the cavity to show the structures & the areas inside it. The following endoscopes are used in gynecological practice.
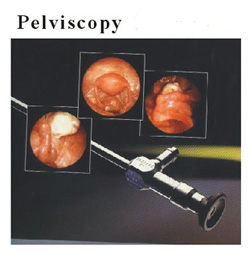
- Pelviscopy to see the pelvic organs
- Hysteroscopy to see inside the uterine cavity.
- Tuboscopy to see inside the fallopian tubes.
- Microcolpohysteroscope is a hysteroscope with magnifications like microscope.
- Colposcope to see inside the vagina is used to detect the lesions of cervix.
Pelviscopy and Hysteroscopy are commonly employed in fertility managements.
Pelviscopy is used for the vision of pelvic cavity. In Fertility practice it is used to assess the health of the reproductive organs; the uterus, the ovaries, oviducts, pelvic surfaces, pelvic peritoneum and to assess the patency of reproductive passages. Ovarian cysts, endometriosis, fibroids, tubal lesions, adhesions, and inflammations can also be seen.
It is also used as therapeutic tool for adhesiolysis, tubal reconstruction, burning of endometriosis, myomectomy, cystectomy and electropuncture of the polycystic ovaries. Technique General anesthesia is usually administered, although it can be performed under a combination of deep sedation and local analgesia. The woman, after undressing is placed on her back with her legs raised in semilithotomy position. A small incision is made just below the umbilicus, a needle passed through it and the abdomen inflated with carbon dioxide. Same incision is enlarged and a trocar and canula introduced through it. The trocar is removed and the Pelviscope passed through the canula. In a new approach, Transvaginal Endoscopy, endoscope is passed through the posterior fornix of vagina and the pelvic organs visualized. |
 |
For assessment of the patency of reproductive passages, methylene blue, a colored dye is injected from the cervix through the canula which has already been placed into the cervix via vagina. If this dye appears in the pelvis as seen through the Pelviscope, the passages will be patent.
Hysteroscopy Uterus is the organ where the pregnancy rests and expands. It is important that uterus is of right size, its cavity is lined with thick favorable endometrium and it has good circulation. Any defect in uterus and its function will make it difficult for the conception to implant and grow.
Since the introduction of ART assessment of uterus has gained immense importance. IVF-ET will not be fruitful if the embryo either fails to implant in the uterus or it is weakly embedded. It is then discharged either at very early stages or there is early pregnancy loss. The whole exercise of IVF is wasted. A fairly good idea of the size of the uterus and its walls is assessed by ultrasound.
|









